A/Prof. Ken Rodgers School of Life Sciences
Learning Objectives
- Discuss, using examples, how maternal drug use may affect fetal growth and development
- Discuss the use of alcohol and tobacco during pregnancy
References
- Rang HP, Dale MM, Ritter JM, Flower RJ and Henderson (2016) Pharmacology, 8th Edition, Churchill Livingstone, Sydney.
- Chapter 57 Harmful effects of drugs
- “A to X: the problem of categorisation of drugs in pregnancy – an Australian perspective” Kennedy, D. MJA 185(10), 2011
Drugs in Pregnancy: Introduction
Physiological changes in pregnancy
- Pregnancy changes:
- Plasma volume increased (increased Vd)
- Maternal plasma albumin concentration is reduced to 70-80%
- decreased protein binding (albumin conc. rises in fetus)
- Cardiac output is increased (increased GFR, liver perfusion)
- GFR increases (increased CL of free drug)
- Estrogen and progesterone alter liver enzyme levels (variable)
- Body fat increases (increased Vd lipid soluble drugs)
- Gastric pH increases
- Pregnancy changes may alter drug distribution and metabolism
- PK and PD changes have not been established for most drugs
Placental transfer of drugs
- Placenta is the organ of exchange between mother and fetus:
- Drug transfer is mainly by diffusion
- Smaller molecules transfer faster
- Less than 500 Da ————› fast
- 600-1,000 Da → slow
- Greater than 1,000 Da will not cross
- Lipophilic drugs cross faster
- Fetal pH more acidic
- So weak acids/bases will become more ionised and tend to accumulate
Drug use in pregnancy
- Pregnant women take an average of 4 drugs during pregnancy
- 40% of these drugs are taken during the critical period associated with teratogenicity
- Pre-conception planning?
Birth Defects
Birth defects are structural or functional abnormalities present at birth that can cause physical disability, intellectual and developmental disability (IDD), and other health problems
Reproductive toxicity testing
- Tests on pregnant animals (rodent + non-rodent eg. rabbit) required for drugs used by women of reproductive age
- Expensive and time-consuming but required by TGA / FDA before licensing
- Main limitation of studies are species differences in metabolism and formation of reactive intermediates
- Spontaneous malformation rate is high (3-10%) and variable between different regions, age groups and classes
- Studies give suggestive rather than conclusive results
Teratogens
Teratogens 1
- Teratogen – a toxic agent that increases the occurrence of a structural defect / abnormality / death (miscarriage) in embryo or fetus after it is administered to:
- the female during pregnancy
- directly to the developing organism
terato = monster, gen = origin
Teratogens 2
- The effect varies, depending upon:
- Amount and length of exposure
- Time of exposure
- Genetic factors (of mother and fetus)
- Additive effects of other teratogens
Teratogens 3
- Teratogenicity is confined to effect of agents on somatic cells (mutagens act on germ cells)
- However teratogens are often mutagens as well
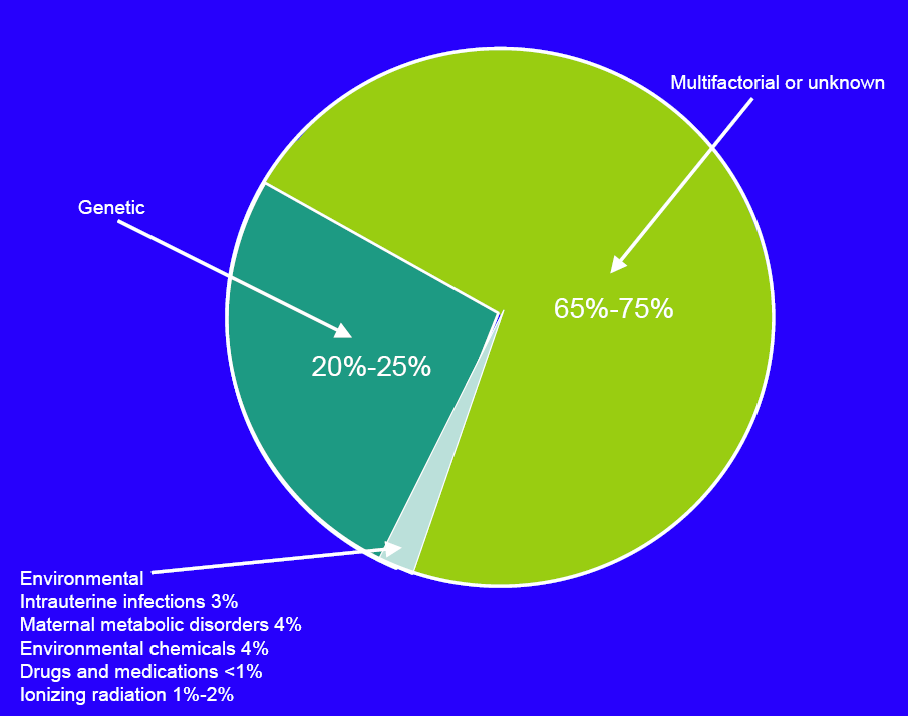
- Majority of birth defects (about 70%) occur with no recognisable causative factor
- Recognised teratogenic agents
- Drug or chemical exposure accounts for about 1% of all fetal malformations (thalidomide, roaccutane, cocaine, alcohol, AEDs)
- Infectious agents (rubella, syphilis, cytomegalovirus)
- Ionising radiation
- Disease (diabetes, lupus, phenylketonuria in mother)
- Genetic
Teratogens 4
- Selectivity
- Most medicines cross the placenta
- Most potent teratogens lack toxicity in mother but produce malformations in fetus rather than death
- However most teratogens will cause death (fetal/maternal) at high enough doses

Teratogens 5




Teratogens 5
- Susceptibility to teratogen is variable
- Blastocyst formation – first 16 days from conception
- resistant to teratogenic effects of medicines but may cause miscarriage
- cytotoxic drugs and ethanol are exceptions
- Organogenesis – day 17 to day 60, critical period of embryonic development when organs start to develop
- susceptible to teratogens eg. thalidomide
- Histogenesis and functional maturation – Beyond day 60, functional changes in organs
- Drugs that interfere with hormones or nutrients inhibit growth or development (not teratogenic)
- eg. renal dysfunction by ACE inhibitors
- Blastocyst formation – first 16 days from conception
Australian Perspective
Australian perspective
- 40% of Australian women reported a chronic health problem during pregnancy (asthma, diabetes)
- 60% of women on medication for chronic problem reported non-adherence to medication due to some concerns
- 30% used complementary or alternative therapies.
- Average age of women having babies is increasing so more likely to be issues with chronic medical conditions (eg hypertension)
- Most practitioners get information from MIMS!!!!
Australian perspective
https://www.tga.gov.au/prescribing-medicines-pregnancy-database

Australian perspective

Australian perspective

Which drugs are used in pregnancy?
- Drugs to treat pregnancy-related conditions such as nausea, constipation, preeclampsia
- Drugs used to treat chronic disorders such as epilepsy, diabetes, asthma and hypertension
- ‘Drugs of abuse’ such as cocaine, alcohol, heroin
Organogenesis & Teratogens
Susceptibility during organogenesis
- The probability of a structural defect is greatest during organogenesis (days 17-60)
- Structural organisation of fetus occurs in a well defined sequence
- Brain
- Heart and major vessels
- Skeleton and limbs
- Ears and eyes
- Palate
- Genitourinary system
- Type of malformation depends on time of exposure
- Structural organisation of fetus occurs in a well defined sequence
Critical period of organogenesis
In the 2 weeks after fertilisation (before full implantation) the embryo might be resistant to teratogenic effects of drugs. No direct communication between maternal and embryonic tissue until after the placenta starts to form.

Teratogens 6
- Specificity
- Different teratogens may give similar abnormalities during same critical periods
- Same teratogen given at different times may produce different effects
- Particular abnormality may represent interference with a specific developmental process
- Net result is reduced cells or cell products at a particular site due to excessive cell death, reduced biosynthesis of DNA, RNA or protein
Teratogens 7
- Access to embryo or fetus
- Drugs/chemicals enter embryonic bloodstream by passive diffusion
- Fetal liver (mid-gestation) has 20-40% of adult activity for Phase 1 reactions
- Embryonic system trapping can occur if
- metabolites are polar
- parent compound/metabolite binds/reacts with proteins
- Prolongs embryonic/fetal exposure
Drugs affecting fetal development

Medicines in Pregnancy
Medicines in pregnancy 1
- Category A
- Taken by a large number of women (pregnant or childbearing age) with no proven increase in frequency of malformations or direct/indirect harmful effects. Controlled studies in women have failed to demonstrate a risk.
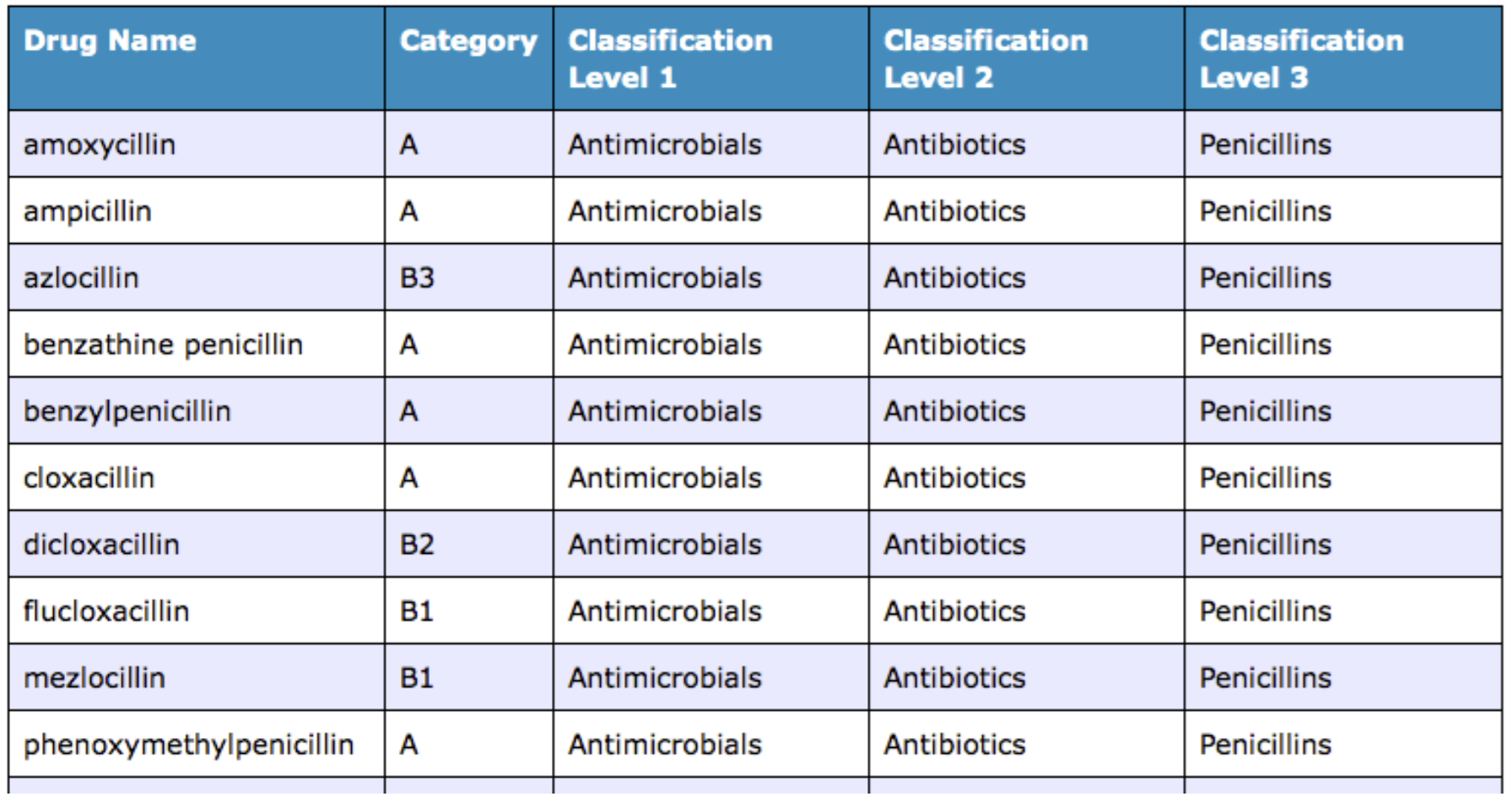
- Category B (50% of Australian drugs)
- Divided into 3 groups (B1, B2, B3) with all having only been taken by limited number of women (pregnant or childbearing age) with no increased incidence of malformation or effects on fetus
- Differences range from no effects in animals (B1) to evidence of fetal damage in animals (B3)
- Category C
- Cause (or suspected) harmful effects without causing malformation – may be reversible OR
- No data available
Medicines in pregnancy 2
- Category D
- Cause (or suspected) increased incidence of fetal malformation or irreversible damage
- but benefits may be acceptable despite risk
- Category X
- Drugs with high risk – not to be used in pregnancy (or possibility of pregnancy)
- Drug is contraindicated in woman who are or may become pregnant
- The allocation to category B does not imply greater safety than category C
- Drugs in category D are not absolutely contraindicated in pregnancy (e.g. anticonvulsants)
Australian perspective

Australian perspective
Medicines in pregnancy 3
- Most medications are assigned to Category C
- This designation indicates that human data are lacking and animal studies were positive or not done
- 66% of all drugs with a pregnancy category are now in Category C
- < 1% of medications have a Category “A” rating, as needs well-controlled human studies
- Despite limited human data on safety in pregnancy and standard label warning to avoid use in pregnancy “unless the benefits outweigh the risks” women are prescribed medications at 38% of visits
Thalidomide
Thalidomide 1
- Specific example: thalidomide
- Effective sedative/hypnotic used by pregnant women, introduced in 1957
- Was originally deemed safe, and often prescribed for nausea and insomnia in pregnant women
- However, it is the cause of severe birth defects when taken in the 1st trimester (100% in weeks 3-6).
- Disturbs the closure of the neural tube and affects brain development.


Thalidomide 2
- Specific example: thalidomide
- Characteristic deformities in virtually 100% of offspring
- amelia (absence of limbs)
- phocomelia (‘seal limbs’; shortening of limbs)
- malformations of face and internal organs
- Up to 10,000 children affected
- Established as human teratogen by William McBride, withdrawn in 1961
- Characteristic deformities in virtually 100% of offspring


Thalidomide 3
Fetal abnormalities in W. Europe

Thalidomide 4
- Specific example: thalidomide
- Had only been tested in mice when marketed
- Difficult to show in experimental animals
- Initially non-toxic in rats
- White rabbits day 8-16, rats only on day 12
- Unidentified metabolite not parent drug appears to be responsible
- Blocks normal development of limbs by preventing angiogenesis
Thalidomide 5
- Specific example: thalidomide
- Lesson: low maternal toxicity and low toxicity in animals may have high teratogenic potential
- Resulted in new drugs being tested in pregnant animals
- Now being re-registered for Rx of cancer and dermatoses (leprosy)
- Anti-angiogenic action
Cigarette Smoking in Pregnancy

Cigarette Smoking
- Largest modifiable risk factor for pregnancy-related morbidity and mortality in US and other developed countries
- Eliminating smoking during pregnancy would reduce infant deaths by 5% and low birth weight infants by 10.4%

Cigarette Smoking
- 20-40% of smokers quit during pregnancy
- Nicotine metabolised more quickly in pregnancy
- May be more difficult to quit
- 60-80% of women who quit return to smoking within a year postpartum
Cigarette Smoking
- Not a major teratogen (? possibly not clear)
- ↓birthweight
- Other obstetric and perinatal complications (eg SIDS)
- Recent study* showed mothers who smoked had a 3x higher risk of having a SIDS case
*Irish Med J. 2012 Apr;105(4):105-8. Maternal smoking and alcohol consumption during pregnancy as risk factors for sudden infant death.
Alcohol Consumption in Pregnancy

Alcohol consumption in pregnancy
Eighty per cent of Australian women drink alcohol during their pregnancy.
Less than one in 100 women drink more than 14 drinks a week.
Foetal alcohol syndrome (FAS)
The adverse effect of ethanol consumption during pregnancy on fetal development was demonstrated in the early 1970s
The features of full FAS include:
- Abnormal facial development, with wide-set eyes, short palpebral fissures and small cheekbones
- reduced cranial circumference
- retarded growth
- mental retardation and behavioural abnormalities, (hyperactivity, poor social integration)
- other anatomical abnormalities (e.g. congenital cardiac abnormalities).
Alcohol-related neurodevelopmental disorder (ARND) v FAS
In ARND there is a lesser degree of impairment than FAS which results in behavioral problems, and cognitive and motor deficits and is often associated with reduced brain size.
Full FAS occurs in about 3 per 1000 live births and affects about 30% of children born to alcoholic mothers. It is rare with mothers who drink less than about 5 units/day, and most common in binge drinkers who sporadically consume much larger amounts, resulting in high peak levels of ethanol.
ARND is about three times as common.
Alcohol consumption in pregnancy
No clearly defined safe threshold, there is no evidence that amounts less than about 2 units/day are harmful.
There is no critical period during pregnancy when ethanol consumption is likely to lead to FAS, although one study suggests that FAS incidence correlates most strongly with ethanol consumption very early in pregnancy, even before pregnancy is recognised, implying that not only pregnant women, but also women who are likely to become pregnant, must be advised not to drink heavily.
Antidepressants Used in Pregnancy

Antidepressant use in pregnancy 1
- As many as 18.4% of pregnant women are depressed during their pregnancy
- As many as 12.7% having an episode of major depression
- Selective serotonin reuptake inhibitor eg Prosac v amitriptyline

Antidepressant use in pregnancy 2
- ~2-fold ↑ risk of cardiac malformations (mainly VSD or ASD) in infants exposed to paroxetine (SSRI) compared with general population (~2% vs. 1%, respectively)
- GlaxoSmithKline retrospective study of pregnant women exposed to paroxetine or other anti-depressants
- Recommendations: If a patient becomes pregnant while taking paroxetine, she should be advised of the potential harm to the fetus. Unless the benefits of paroxetine to the mother justify continuing treatment, consideration should be given to either discontinuing paroxetine therapy or switching to another antidepressant in these cases.

Antidepressant use in pregnancy 3
- Neonatal Abstinence Syndrome (NAS)
- Symptoms of NAS present in 18 of 60 (30%) SSRI-exposed infants versus none of 60 control infants (p<0.001)
- Peak symptoms within 1st 48 hours
Antidepressant use in pregnancy 4
- Risks of Untreated Depression during Pregnancy
- Suicidal ideation
- Substance abuse
- Spontaneous abortion
- Preeclampsia
- Preterm delivery and low birth weight
- Neonatal neurobehavioral effects
- Postpartum depression
Can J Psychiatry 2004;49:726-35
Risk vs. Benefit Assessment
– Health of mother affects the health of fetus
– Conditions threatening mothers health need to be addressed (eg asthma)
– FDA retrospective study on drugs and adverse outcomes
In some pregnant women it may be necessary to continue medication
