A/Prof. Ken Rodgers School of Life Sciences
Learning Objectives
- Describe the influence of thevolume of distribution on tissue distribution of drugs
- Utilise the volume of distribution to calculate body burden, verify quantities of drug ingested* and calculate peak plasma concentrations
- Explain the role of plasma proteins in modulating free drug plasma concentrationsand to determine drug half-life
- Explain the risks associated with displacement of plasma protein-bound drugs#
*If you know the volume of distribution of a drug you can predict the total amount of drug in the body based on the plasma concentration. This is important in an overdose situation
#This is only clinically important when drugs are highly protein bound
References
- Rang HP, Dale MM, Ritter JM, Flower R and Henderson G (2016) Pharmacology, 8th Edition, Churchill Livingstone, Sydney.
- Drug absorption and distribution– Chapter 8
Drug distribution
Drug distribution 1
- Once drugs are absorbed into the blood they can diffuse into different compartments in the body. The equilibrium pattern of distribution of the drug between the various compartments in body depends on:
- Permeability across barriers (lipid bilayers)
- Binding within compartments (this can result in a higher concentration of drug in this compartment)
- pH partition (degree of ionisation can change – remember the pH changes)
- Fat:water partition (lipid solubility)
Drug distribution 2
Drugs that are strongly protein bound stay mainly in the plasma compartment (~ 3L)
Lipid-insoluble drugs are mainly confined to the plasma and extracellular fluidsmost don’t enter the brain (~ 15L)
Lipid-soluble drugs reach all compartments and may accumulate in fat (~40L)
Plasma Protein Binding

Plasma protein binding 1
- Plasma proteins
- a) Albumin – binds slightly water soluble drugs (weak acids/bases)
- most important of all PP (50-60% of total plasma proteins)
- two binding sites per albumin molecule
- a) Albumin – binds slightly water soluble drugs (weak acids/bases)
- b) α1-acid glycoprotein and β-globulins – less important (binds mainly weak bases)
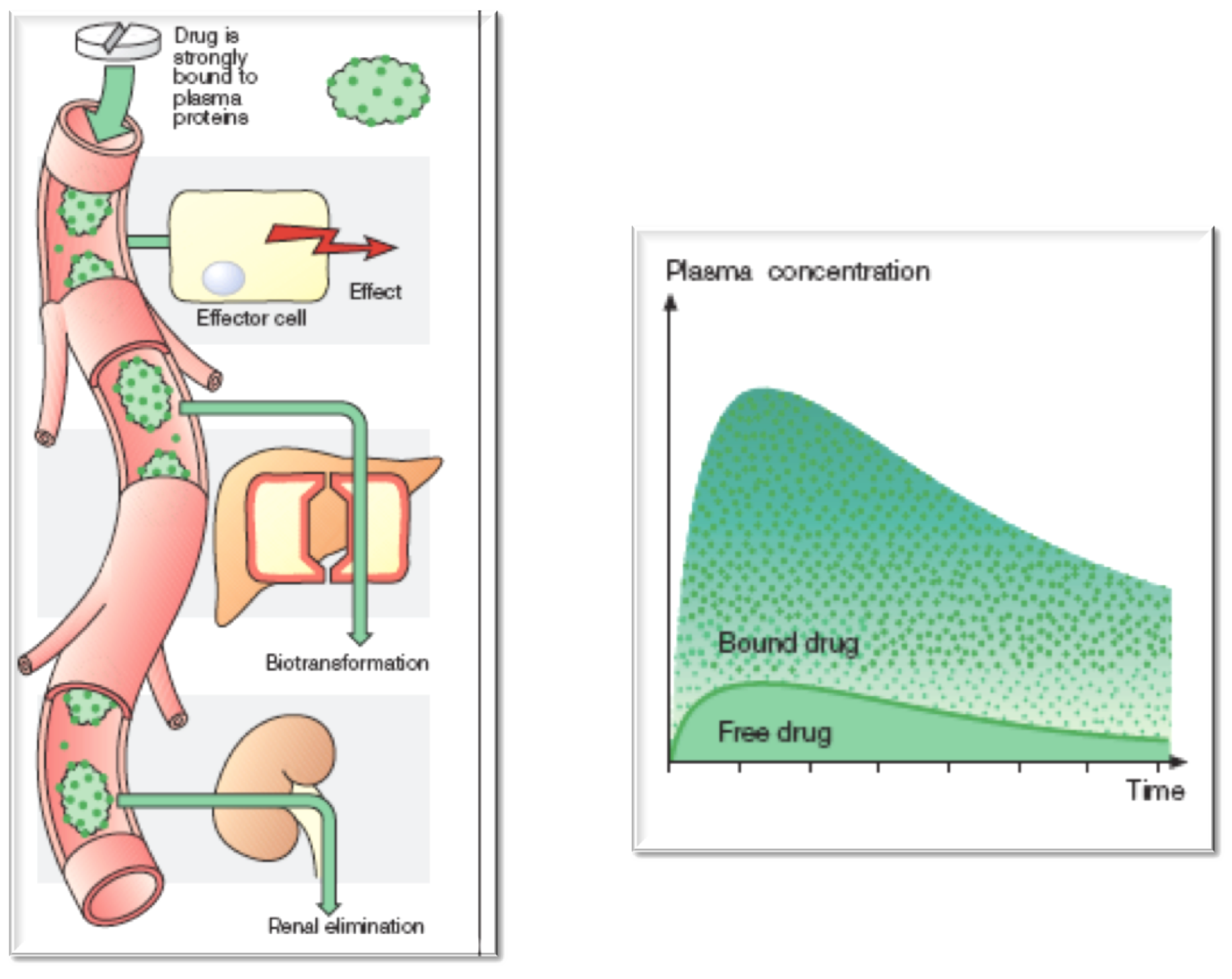
Plasma protein binding 2
- Many drugs are bound to plasma proteins
- There is an equilibrium between bound and free


Drugs with low affinity for plasma proteins

Drugs with high affinity for plasma proteins
Extent of plasma protein binding
- If the free fraction (FF, unbound) is <10% apparently slight variations in FF can have important consequences: potential for drug interactions
- As FF becomes larger (eg 10-25%) binding becomes less important



Plasma protein binding 4
- Most assay systems measure total (free + bound) drug concentrations (Note: only free drug is active)
- Binding capacity of albumin is up to 1.2 mM so at normal doses most drugs are not saturated
- But some drugs work at Cp close to saturation point eg. sulphonamides, tolbutamide, phenylbutazone
- Extensive PP binding can result in greater than expected rises in Cp following small increases in dose


Plasma protein binding 3
- If two drugs compete for the same site then stronger affinity will transiently displace weaker affinity
- bilirubin displaced by sulfonamides in children → crosses BBB → kernicterus (choreoathetosis – permanent movement disorder)
- Especially important if they also reduce elimination
- phenylbutazone displaces warfarin and also inhibits warfarin metabolism → internal bleeding
- aspirin displaces methotrexate and also reduces its renal secretion → GIT and kidney toxicity
- quinidine/verapamil/amiodarone displace digoxin and reduce its renal excretion → severe dysrhythmias

Factors affecting plasma binding
- Other factors can increase free drug concentrations leading to potential toxicity

Binding to tissue components
- Drug reservoirs
- Thiopentone in fat
- prolonged anaesthesia following repeated doses (limits use to short-term induction agent)
- Tetracycline in bone / teeth
- discolouration of teeth, brittle bones in children (not given to children, pregnant/breastfeeding women)
- Chloroquine in melanin granules in retina
- retinopathy
- Carbon monoxide on RBC haemaglobin
- asphyxia
Volume of Distribution: Definitions
Volume of distribution definition
- Defined as the the volume of fluid required to contain the total amount of drug (Q) in the body at the concentration present in plasma (Cp)
- Apparent volume of distribution (Vd) is a parameter used to estimate how widely distributed the drug is in the body
- This is important because not all drugs distribute equally throughout all body fluids
- only plasma (3 L in a 75 kg man; 0.04 L/kg)
- all extracellular fluid (=12 L; 0.17 L/kg) but not intracellular fluid
- total body water (=41 L; 0.59 L/kg)
The main body fluid compartments


Volume of Distribution: Calculations
Calculating the volume of distribution
- Analogous to putting a known amount of drug (100mg) in a beaker of unknown volume (?), then measuring the concentration of drug (2mg/ml)







Calculating the loading dose
- Analogous to putting a known volume of water (50ml) in a beaker and adding enough drug to give a solution 2mg/ml.








Volume of distribution 2
Q = Quantity of drug (mg or g) in the body
Vd = Volume of distribution
Cp = Concentration in plasma
Can also be used to calculate loading dose
Loading dose = target conc. x Vd

Volume of distribution analogy

Volume of distribution
- Assumptions:
- 1. The drug must be instantaneously distributed and no metabolism should have occurred
- 2. No portion of the drug should have been excreted
- 3. No portion of the drug should have been sequestered (thiopentone, being lipid soluble is sequestered into fat)
Volume of distribution
- Vd is a constant for each compound
- If tightly bound to plasma proteins or is very ionised, Vd will be close to blood volumes (3L)
- If bound by tissues, drug will appear to be dissolved in a large volume and Vd will be large (>>3L)
- [plasma] relatively low for a given dose
- Likely to be concentrated in body fat (or other tissue)
- Likely to cross the blood–brain barrier
- Likely to have a longer half-life in the body
Volume of distribution 6
Use the following formula to calculate the Vd for the above drugs.
For ethanol you will need to know that the density is 0.78 g/ml



Volume of distribution calculations
DYE: Vd = 100g divided by 33g/L = 3L
ACETAZOLAMIDE: Vd= 100mg divided by 8mg/L = 12.5L
ETHANOL: Density is 0.78g/ml so 64ml = 50g
Vd = 50g divided by 1.56g/L = 32L
IMIPRAMINE: Vd= 100mg divided by 0.225mg/L = 444L

Volume of distribution uses
Uses
- Can be used to calculate loading dose
- Predict likely rate of excretion
- Determining body burden (total amt. of compound in body = Cp.Vd)
- Verify history of quantity of drug ingested
Q&A
Volume of distribution question
Example
- A child and an adult ingest two Lanoxin® 250µg tablets (Rx atrial fibrillation and HF)
- The Vd of Digoxin is 7 L/kg
- The child weights 12kg and the adult weighs 70kg
- What are the peak plasma concentrations in the adult and the child?
Volume of distribution answer
- Example
- Child and adult ingest digoxin(Rx atrial fibrillation and HF)
- Digoxin Vd = 7 L/kg, What is the peak [plasma]?


Drug distribution
- Drugs leave the body mainly through the:
- Kidneys
- Most drugs excreted in the urine (unchanged/metabolites)
- Lungs
- Only highly volatile/gaseous agents (eg isoflurane, desflurane)
- Biliary system
- Few secreted in the bile (eg rifampicin, vecuronium, morphine)
- Becomes important in renal failure (eg digoxin)
- (Breast milk)
- Negligible – only important due to effects on newborns (eg atenolol, caffeine, fluoxetine, phenobarbitone, cocaine)
Question 1
1. You need to give a patient (100 kg) a loading dose of drug X by a single I.V. injection, prior to commencing an I.V. infusion. The required plasma concentration of drug X is 10 mg/litre. The apparent volume of distribution (Vd) of drug X is 0.05 litres/kg, What loading dose of drug X will most closely reach this concentration?
(A) 2 mg
(B) 10 mg
(C) 20 mg
(D) 50 mg
(E) not enough information
Answer to question 1
- 1. You need to give a patient (100 kg) a loading dose of drug X by a single I.V. injection, prior to commencing an I.V. infusion. The required plasma concentration of drug X is 10 mg/litre. The apparent volume of distribution (Vd) of drug X is 0.05 litres/kg, What loading dose of drug X will most closely reach this concentration?
The volume of distribution is 0.05 litres per kg – since the patient is 100kg the volume of distribution is 5 litres (100 x 0.05)
To calculate the loading dose use the formula:
Loading dose = target conc. x Vd
So loading dose = 10mg/litre x 5 litres
= 50 mg
(the ‘litres’ on the top and bottom of the equation cancel out)